0.1. Scheme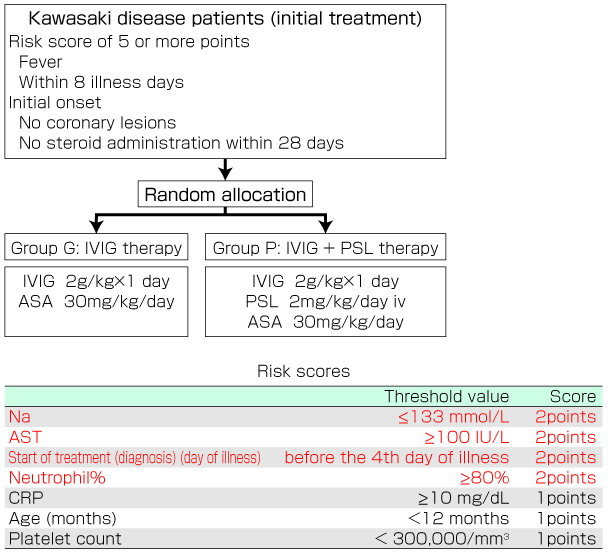 0.2. PurposeConduct randomized controlled trial to test the hypothesis that initial high-dose immunoglobulin plus prednisolone combination therapy is superior to standard high-dose immunoglobulin treatment for patients with severe (risk score, ≥5 points) Kawasaki disease. 0.3. EndpointsFrequency of coronary lesions occurring during the trial is the primary endpoint. The secondary endpoints are frequency of coronary lesions at 4 weeks after the start of treatment; Z-scores for the main trunks of the right and left coronary arteries and their anterior descending branches; percentage of patients refractory to treatment; number of days from start of treatment to end of fever; CRP levels at 1 and 2 weeks after start of treatment; and frequency of adverse drug reactions. Echocardiographic findings before registration, and at 1, 2, and 4 weeks after start 0.4. Criteria for inclusion and exclusion1) severe Kawasaki disease (risk score, ≥5 points)2) accompanied by fever 3) Kawasaki disease diagnosed within 8 days of illness 4) no coronary lesions as a complication before registration (echocardiogram) 5) no past history of Kawasaki disease 6) no disease resembling Kawasaki disease 7) no active, severe, bacterial infection as a complication 8) no steroid use in the previous 28 days either orally, or through intravenous, muscular, or subcutaneous injection 9) no intravenous injection of gamma globulin in the previous 180 days 10) no serious underlying diseases or disorders 11) written consent to participate in this study obtained from either the patient's family or the patient 0.5. TreatmentGroup G: High-dose immunoglobulin therapy (IVIG therapy)
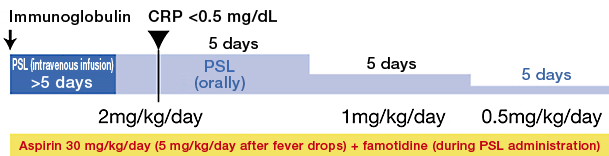
Group P: High-dose immunoglobulin therapy plus prednisolone therapy (IVIG + PSL therapy)
The maximum dose of PSL is 60 mg/day. Therefore, if a patient weighs more than 30 kg, reduce the PSL dose as follows: 60 mg/day --> 30 mg/day --> 15 mg/day. 0.6. Planned number of registered patients and research periodProjected number of registered patients: 392 0.7. InquiriesTo request information on registration procedures or clinical decision-making (eg, indication criteria, criteria for changing treatment), contact the Study Secretariat |
|||||
|
|||||
| RAISE Study Group The Ministry of Health, Labour and Welfare (MHLW) general research project to commercialize medical technology A prospective, randomized, controlled study for examining the efficacy of initial immunoglobulin plus prednisolone combination therapy for severe Kawasaki disease |
|||||